Health Care Systems
Health care systems organise the finance and delivery of health care. They vary by country, reflecting specific history, culture, and economics. To maximise coverage and efficiency they must evolve with changing demographics, needs, and technologies.

An eye on sustainability at the Economist’s Future of Health Europe
30 October 2023
Learn more about how the topic of sustainability was tackled by a broad range of speakers and the key themes which emerged.
Grow and diversify funding for prevention to boost the nation’s health and prosperity, urges landmark report
12 October 2023
Our new report examines the promise of prevention in healthcare and provides six key recommendations that could usher in a new era of optimised prevention.
Reimagining Prevention for a Healthier, More Prosperous Society
12 October 2023
In this report, we highlight the significance of prevention as a cost-effective and often cost-saving investment for public sector resources. Prevention, covering primary, secondary, and tertiary measures, can help to reduce ill health, improve healthcare capacity, and increase wider economic growth.
The Economics of Health in a Shifting Climate: Insights from the 2023 Annual Lecture
26 September 2023
OHE invited Climate Change Economist, Professor Elizabeth Robinson to give the 2023 Lecture at the Royal Society of Medicine. She used the opportunity to demonstrate the importance of a one health perspective when transitioning into a climate-resilient future.

Partnerships for Health System Innovation and Improvement
31 August 2023
Many countries around the world are experiencing strains on their healthcare systems. Innovation has the potential to support healthcare systems to strive for improved productivity to…

The changing role of the NHS over time
14 August 2023
OHE has been producing reports since 1962 which give insights into issues facing the NHS in the 75 years since it was created. The first part…
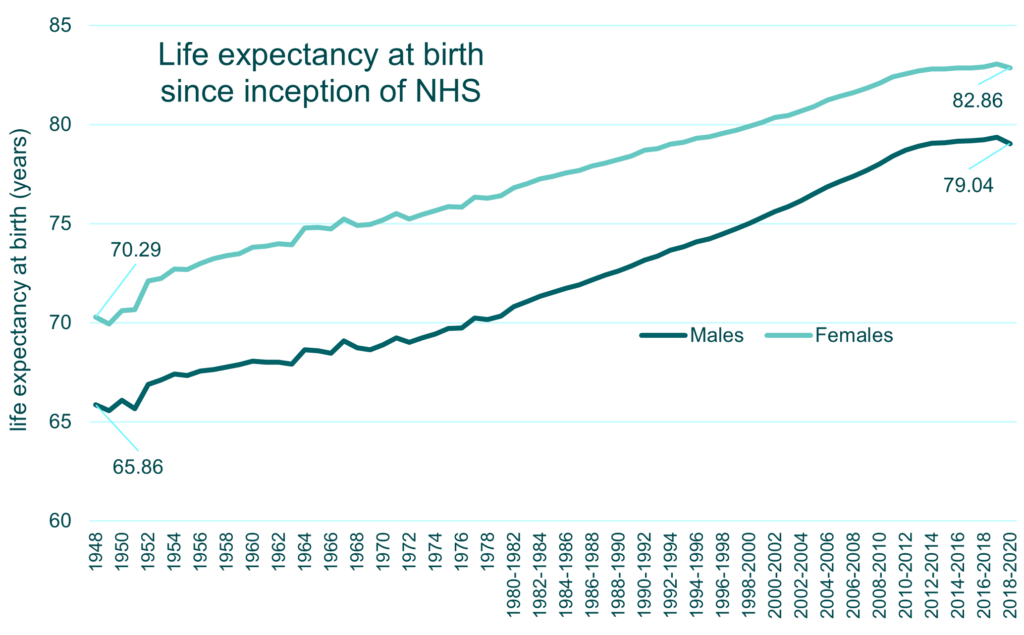
Can a continued focus on prevention, diagnosis, and treatment see the NHS to another 75 years?
27 July 2023
We have delved into the OHE archives to reflect on past NHS successes. In part one of a two-part Insight series, we look at three major contributors to shorter life expectancies – tuberculosis, heart disease, and cancer.

A Prescription for Green Healthcare Delivery: Insights from an Expert Sustainability Webinar
19 July 2023
OHE delivered a webinar on pharmaceutical sustainability, supported by ABPI, bringing together leading experts and professionals from government, healthcare, and industry. This webinar builds on a recently published OHE report on sustainability in the pharmaceutical industry.

Caring about Carers: Improving Consideration of the Burden of Informal Caring in HTA
11 April 2023
Through a three-part webinar series, commissioned and funded by Roche, OHE has explored the burdens on informal carers when providing unpaid care for loved ones.